
Energy, from First Principles
Mitochondria

Sentence
Mitochondria is the powerhouse of the cell. Don’t mess with the powerhouse unless you’re sure you know what you’re doing.
Paragraphs
Energy creation is fundamental to life, and mitochondria are essential to energy production. To understand health from first principles, it is essential to understand how the body fulfills this fundamental process. It stands to reason that in order to optimize performance and longevity, one should optimize mitochondrial function.
To optimize mitochondrial function, it’s important to understand how they do what they do. Mitochondria are organelles, or one of many working parts of a cell. A cell can have varying amounts of mitochondria, depending on its function. Organs that require a lot of energy generally have cells with a lot of mitochondria. Through a complex but elegant process, mitochondria generate ATP, a molecule with high energy bonds that can be used elsewhere in the cell to carry out essential processes.
The first step in ATP production is breaking down or converting the food we eat to glucose. Glucose is then broken in half and enters the Krebs cycle. The Krebs cycle produces a small amount of ATP, but more importantly two types of byproducts (NADH and FADH2) that are then fed into the electron transport chain to produce more ATP. Making sure the mitochondria have what they need to carry out this process is the first step to health.
More importantly, though, is to make sure we’re not unintentionally impeding mitochondrial function. We can extend and specify the Hippocratic Oath in this instance to “Do no harm to mitochondria.” Unfortunately, there are a number of prescription medicines that do exactly that, but very rarely are the direct effects on mitochondrial function considered when prescribing a medicine. This is a very undervalued risk when contemplating the risk/reward benefit of a medication.
The full essay and its accompanying audio recording are available to paid subscribers only.
MITOCHONDRIA: FIRST PRINCIPLES OF ENERGY
Energy is essential to life. Mitochondria are essential to energy. Because of this, they are absolutely fundamental to our health. Everyone knows they are the powerhouse of the cell. There is no question about their importance in theory. In practice, though, rather than being the primary focus, mitochondrial health is often ignored. Mitochondrial dysfunction plays a role in a wide range of diseases (maybe even every disease), ranging from metabolic syndromes to likely contributing to mental health issues (which probably have metabolic underpinnings), and are a primary driver of ageing in general. Whenever we talk about “metabolism”, we are talking about mitochondrial function, because they are the fundamental level at which metabolism takes place. In studying health and sickness from first principles, there is no better place to start than with mitochondria.
The reason we eat is to provide fuel for mitochondria, and the reason we breathe is to remove the byproducts of mitochondrial processes. It doesn’t get much more fundamental than this. Mitochondria supply over 90% of the energy our body needs to function, so any wide-ranging impairment in their function will be significant, even if it’s not immediately noticeable. They are present in greater density in energy-intensive organs, such as the brain, heart, skeletal muscle, liver, and kidneys. It stands to reason, then, that these organs would be disproportionately affected if mitochondrial efficiency decreased. Mitochondria do have other functions as well, but we will focus on energy for now.
Adenosine triphosphate (ATP) is the fundamental molecule the body uses to store energy and it is often referred to as the “energy currency” of the cell. When energy to perform a function is needed, the high energy bond holding the phosphates together is broken, which results in a release of energy and a molecule that is now adenosine diphosphate (ADP). Most ATP generated from the breakdown of food takes place in the mitochondria.
Most carbohydrates in our diet can be broken down into the simple sugar glucose, a six-carbon molecule, which is the primary starting point for energy production at the cellular level. There are other simple sugars, but they can either be converted to glucose or implemented into other areas of the energy production cycle. Protein can also be broken down and reconstituted into glucose molecules if carbohydrates are absent from the diet.
The process of turning glucose into usable energy occurs through the Tricarboxylic Acid Cycle, also known as the TCA, Citric Acid, or Krebs cycle. The TCA cycle occurs inside the mitochondria.
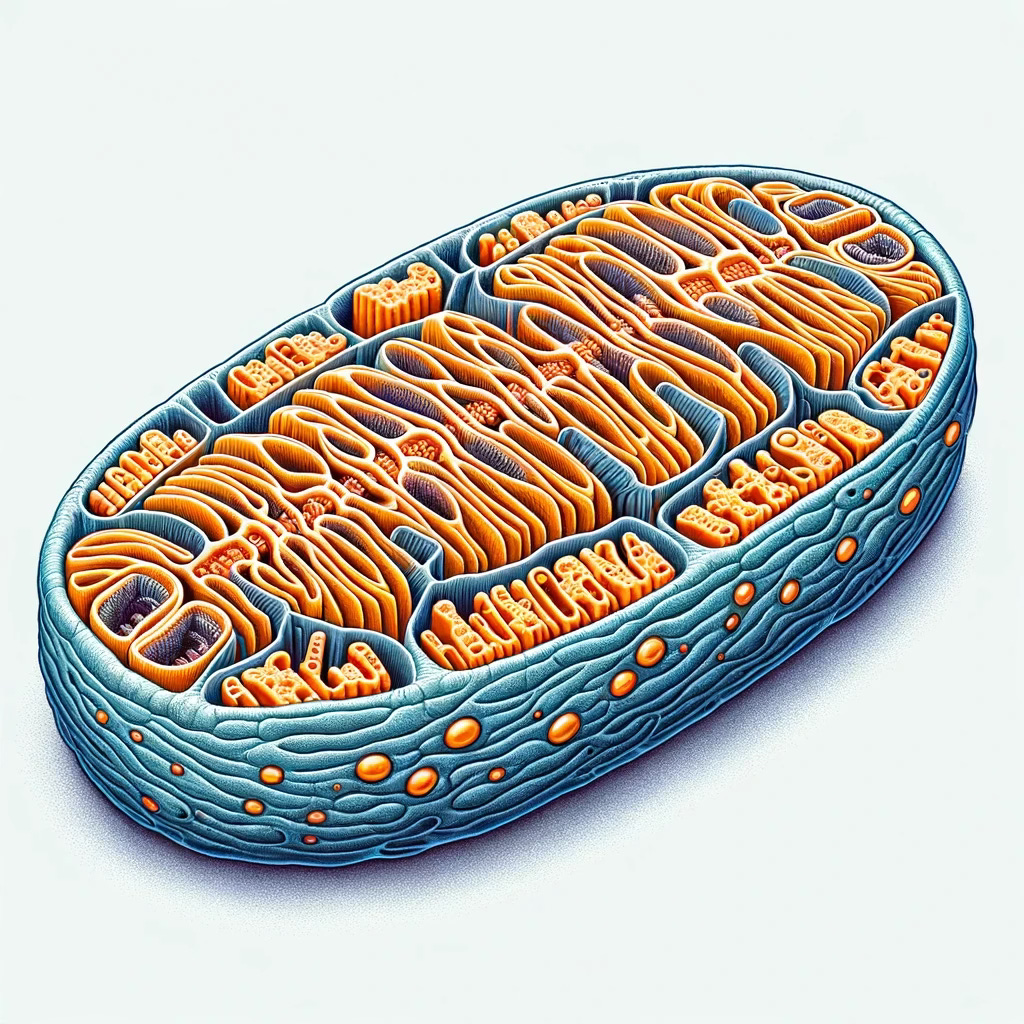
Mitochondria are small structures within a cell that are thought to have once been independent organisms, but at some point in our evolutionary past merged with a eukaryotic cell and developed a symbiotic relationship in which mitochondria helped provide more energy for the cell to grow and divide. (When we say merged, we mean eaten, but then somehow avoided destruction.) Mitochondria interestingly have retained some of their own DNA separate from the rest of the cell, but have exported most of their genetic information to the cell nucleus for safekeeping.
Mitochondria have an outer membrane and an inner membrane. Inside the inner membrane is the matrix, and that is where the TCA cycle takes place. If you think of an inflatable kiddie pool, the matrix is where you put the water in the pool. The TCA cycle itself doesn’t produce much ATP, but some of the molecular byproducts (NADH and FADH2) then undergo oxidative phosphorylation to create more ATP.
Oxidative phosphorylation involves breaking apart these molecules and capturing the released electrons. The electrons are then passed along the Electron Transport Chain (which consists of proteins embedded along the mitochondria’s inner membrane) like a game of hot potato. With each passing of the negatively charged electron, a positively charged hydrogen atom is pumped from the matrix of the mitochondria to the other side of the inner membrane. (This would be like the air-filled walls of the kiddie pool.) As these hydrogen atoms and their positive charge build up outside the inner membrane, they naturally want to move back to the matrix to balance out the electrical charge on each side of the inner membrane. You can think about it as water pushing against a dam. And just like a dam, the hydrogen atoms are funneled back to the matrix through a protein that is essentially a turbine, and with each spin a molecule of ATP is created.
This is a very simplified explanation but will suffice for now. It should be noted that ATP creation isn’t 100% efficient (not every proton flowing through the turbine creates one ATP) and efficiency will vary between people. The efficiency level is known as the mitochondrial coupling rate. Also, in addition to producing needed ATP, this process also creates unwanted byproducts called Reactive Oxygen Species (ROS). Much like their near-homonymous RUS (rodents of unusual size), ROS scurry around the cell and cause damage to other structures unless they are properly controlled. Mitochondria have a number of mechanisms to combat this, but it’s not perfect and the slow destruction over time by ROS is implicated in decreasing mitochondrial function over time leading to disease and many of the symptoms which we associated with ageing.
The importance of mitochondria is undeniable, and their importance is evident in the scientific literature. Searching “mitochondria” on PubMed returns over 250,000 papers. 6,000 papers in 2011 alone were published about mitochondria, but mitochondria are quickly forgotten and overlooked in everyday discussions about health and medicine. When’s the last time you talked with your doctor about mitochondrial health? If it’s essential in the fundamental process upon which almost all health and disease is based, it probably should come up once in a while. In medical school, mitochondria are usually discussed during the small first year section of cell biology, and then only reappear later in discussion of rare mitochondrial diseases such as MELAS, MIDD, MERFF, and LHON. It’s also unfortunate that any internet deep dive into mitochondria almost instantly leads down a rabbit hole of pseudo-medicine. Mitochondrial health should be a primary concern of any practical or clinical medical practice.
Mitochondrial Health
Since mitochondrial health is so important to literally every aspect of our life, we’ll go through in some detail about how to improve/optimize mitochondrial function.
Exercise
First and foremost, exercise is essential in both increasing both the amount and efficiency of mitochondria. Regular exercise is the best way to increase overall energy levels, specifically because of its effect on mitochondria. Exercise has been shown to increase mitochondrial density not only in skeletal muscles, but also in the heart and brain1,2. Any exercise is better than no exercise, but the optimal exercise regimen consists of what is considered Zone 2 training with brief episodes of high intensity exercise.
Exact definitions vary, but zone 2 is generally considered to be around 60-70% of your maximum heart rate. Again, calculations to estimate maximum heart rate differ, but a simple formula is 220- your age. If you’re 40 years old, your estimated max heart rate would be 180 and your zone 2 range is 108-126. Another way to judge if you are in zone 2 is if you were talking to someone on the phone, you could respond in full sentences, but the person on the other end could tell you were exercising. This is also what is considered “moderate” exercise.
The reason zone 2 is important to mitochondrial health is it represents the level at which mitochondria are operating at their maximal efficiency. Zone 2 is also considered the intensity level you could theoretically maintain for a full day. This is because mitochondria are processing lactate, a byproduct of anaerobic exercise, at the same rate as it’s being produced, preventing it from building up in your muscles.
Intense exercise, zone 5, or 90+% of max heart rate, puts the greatest energy demand on the cells, thus signaling to the cell that it needs more mitochondria and stimulating mitochondrial biogenesis. (Inigo San-Millan is the prominent figure in this area of research, and his various appearances of podcasts are always fascinating.) General medical guidelines are 150 minutes of moderate exercise a week, or in other words, 30 minutes 5 days a week of zone 2 training. This should be considered a minimum. Dr. San-Millan’s recommendations (from his podcast with Peter Attia) are 4 days of zone 2 training for 60-90 minutes and one day of zone 5 training, which is shorter, but far more intense.
Fuel
The next step is to ensure the mitochondria have the fuel they need to function and produce ATP. Food that is broken down to glucose is the substrate that enters the TCA cycle and kicks off the process of generating ATP, but this process has its own requirements. We’ll highlight a few of the more important ones below:
Iron
Iron acts as an electron carrier in the Electron Transport Chain (ETC). (It plays the hot potato game passing electrons along.) Studies in iron-deficient (but non-anemic) athletes showed definitive improvement in mitochondrial functioning with iron supplementation3 and generally showed increased endurance. (Their non-anemic status is important, because a common manifestation of low iron is anemia, or too few red blood cells (RBCs). If the subjects were anemic, replacing iron would help increase RBC count and that would also improve performance, confounding the results. Isolating the non-anemic patients helps point towards increased mitochondrial function being the primary driver of athletic improvement rather than just increased RBCs.) An iron panel blood draw can show your iron status. There’s not much literature on improved energy efficiency in people with normal iron levels, but your internal energy production line is not functioning at full capacity if you are in an iron deficient state. Most meats and seafood are rich in iron, as are dark leafy greens, but absorption from animal products is generally greater compared to plants.
Magnesium
Magnesium is an essential co-factor for many steps in the TCA cycle (and over 600 other processes in the body). Chronic magnesium deficiency is starting to be implicated in the development of many metabolic disorders, including obesity, type 2 diabetes, hypertension, and others. Remember, when you read/hear metabolism, think mitochondria. Again, magnesium supplementation has been shown to increase exercise and muscle performance and in decreasing lactate buildup (indicating mitochondria are functioning efficiently). Unlike iron, simple blood tests don’t give an accurate representation of the body’s magnesium status because <1% of magnesium in the body is in the blood. There are other measurement options, but none of them are great ways to measure magnesium levels. An average diet supplies only about 50% of needed magnesium. This is partly due to food selection, but also magnesium levels in food itself is decreased due to declining soil quality. Foods groups high in magnesium include nuts, seeds, beans, avocados, leafy greens and whole grains.
Since the body’s magnesium status is somewhat of a black box, and it’s very hard to get sufficient magnesium through diet, supplementation is likely helpful. The body generally does a good job of only absorbing the magnesium it needs. If its stores are full, less gets absorbed from the intestine. Some magnesium is excreted through the kidneys daily, so magnesium is regularly needed to replace losses. Exercise also increases the need for magnesium. Again, the body manages magnesium levels well, so your job is to make sure enough magnesium is available to be absorbed when needed. (Quick side note: One side effect of magnesium can be loose and/ or urgent bowel movements, and the less that is absorbed, the more remains in the gut to cause these side effects. So, if you’re overdoing the magnesium, it can be uncomfortable.) Magnesium recommendations are 400-420 mg daily for men and 300-320 mg for women. Making sure you are getting plenty of magnesium is a good way to make sure your mitochondria have what they need to function.
Coenzyme Q10, aka CoQ10, aka Ubiquinone
CoQ10 also acts as an electron carrier in the ETC and has antioxidant properties, which protects the mitochondria from the pesky ROS they are constantly producing. It has many other roles, and the name ubiquinone was given because of its ubiquitous presence throughout the body. Like magnesium, it’s difficult to assess the body’s overall CoQ10 state through blood testing. While it is essential to mitochondrial function, supplementation of CoQ10 has inconsistent benefits in any measurable outcomes when it comes to exercise performance, VO2 max (a measure of maximal exercise capacity), or recovery. Some studies showed benefit, but the majority did not4. It can be helpful in mitigating side effects of statin medications (more on this below), but in an otherwise healthy person, it probably doesn’t provide much value.
The body can synthesize CoQ10, but not in sufficient quantities for optimal functioning. Foods high in CoQ10 include meats and fish, especially organ meats. It is found in some vegetables, but most vegetarians will likely be CoQ10 deficient4. If you choose to supplement CoQ10, ubiquinol is much better absorbed than ubiquinone.
Glutathione
As discussed earlier, the energy production process results in toxic byproducts that can wreak havoc within the mitochondria. Mitochondrial damage will be discussed in more detail below, but glutathione is the most important molecule in helping neutralize the toxic ROS and protecting mitochondrial function. Glutathione is rarely tested for in the clinical setting and is primarily reserved for research studies. Glutathione is synthesized in the body, and its precursors include glycine and cysteine. Studies have shown that supplementation with these building blocks with glycine and N-acetyl cysteine (GlyNAC) did increase glutathione levels in the blood and it did correlate with increased exercise capacity, strength, and gait speed (in older adults) and decreased inflammatory markers.
Manganese, vitamins B1, B2, and B3, carnitine, riboflavin, and niacin are all also necessary for mitochondrial function, but play lesser roles, so we’re not going to dive into them here.
In conclusion, to optimize mitochondrial function, iron levels need to be in a normal range, supplementing with magnesium and glutathione precursors is probably helpful, and although CoQ10 is essential, supplementing likely won’t produce measurable benefit except in the case of taking statin medications.
Mitochondrial Damage
Mitochondrial dysfunction is demonstrable in a wide range of diseases including all metabolic diseases (obesity, type 2 diabetes, hyperlipidemia, NAFLD, etc.), Alzheimer’s, Parkinson’s, autism, cardiomyopathy, and chronic kidney disease. There are specific mitochondrial diseases, such as MERFF, MELAS, and LHON, which although sound like they could be names of your multiethnic neighbors in a Boston apartment building, are serious crippling diseases. They come with a range of symptoms, but consistent with the logic that cell types with the highest number of mitochondria will be affected the most, they tend to affect the brain, eyes, muscle, and heart.
Decreased efficiency of mitochondrial function can come from genetic causes or acquired over time from accumulated damage. Mitochondria are essentially inherited only from the mother. Egg cells have far more mitochondria than sperm, so when the two fuse to form an embryo, the mitochondria present are almost solely from the mother. Because of this, genetic mitochondrial diseases pass from a mother to her children.
Because of the hazardous waste products (ROS) emitted by the ATP-generating process, mitochondria inevitably sustain damage. There are several protective mechanisms, but they are imperfect. This gradual accumulation of damage is considered a fundamental aspect of the overall process of aging, in addition to development of specific diseases. It’s also important to note that these ROS emissions aren’t all bad. Their presence can trigger beneficial changes, mostly in helping the body adapt to stress, and are used by immune system cells to kill invading bacteria.
To maintain our focus on the energy-producing and fundamental importance of mitochondria, we won’t delve deep into any of those processes at this point. The purpose here isn’t to discuss each individual disease, but in future essays about each condition, mitochondrial function will be a primary focus.
In the same way we try to optimize mitochondrial function, we should avoid unnecessary inhibitors of their functions. Avoiding harm is actually far more important than anything that can be done to optimize their function. Many medications, both prescription and non-prescription, have unintended effects on mitochondria and these effects are often overlooked or ignored. Again, since mitochondrial function is absolutely essential to life and health, medication effects on mitochondria should be our foremost concern and an essential consideration in any risk/benefit discussion.
Statins
Statin medications are commonly prescribed for dyslipidemia, or high cholesterol, with the intent to reduce risk of heart attack or stroke. By commonly prescribed, we mean that atorvastatin (Lipitor) is the most prescribed medication in the United States and the highest grossing prescription drug of all time, generating over $163 billion in sales for Pfizer as of 2021.
Statins directly affect mitochondria by inhibiting an enzyme called HMG-CoA reductase, which is involved in cholesterol synthesis. It’s also involved in the production of CoQ10. Without CoQ10, the ETC doesn’t function as it should and ROS build up in the cell, increasing levels of damage. The drug also appears to affect the complexes of the ETC and decrease mitochondrial biogenesis, or the creation of new mitochondria.
Because of this direct action, statins have high rates of side effects. These side effects are generally mild and preferrable to a heart attack, but there are undeniable incentives to both minimize perception of its harms and overstate the risk reduction. Starting a statin should be a conversation with your primary care doctor, but any method or lifestyle intervention to reduce cardiovascular risk should first be implemented. Sure, starting a medication to lower cholesterol is far easier, but it comes with its own risks, which are often understated.
Consistent with the theory that organs with high levels of mitochondria will be most affected by injuries to mitochondria, the most common side effects of statins are joint and muscle pains, brain fog and insomnia, and elevation of liver enzymes. (Muscles, brain, and liver all have high mitochondrial density.) A medication that directly impairs the functioning of mitochondria, the fundamental driver of energy and life, should be treated with the upmost caution.
When starting a statin for primary prevention of cardiovascular events, the rationale is based off the levels of total and HDL cholesterol (and the subsequent calculation of LDL based off those two numbers), blood pressure, and other lifestyle and genetic factors. This information is plugged into a risk calculator, which then provides a 10-year risk assessment of the patient’s likelihood of severe cardiovascular event, like a heart attack or stroke. The guidelines for starting a statin are based off total LDL levels and this risk assessment.
Put another way, the risk you’re trying to decrease stretches across the next decade. The annual risk (year by year risk) is weighted towards the back end of that decade, since age itself is a major driver of the heart attack risk. (If your 10 year risk is 10%, that’s about 1% per year, but it’s less than one percent in the first years, and slightly greater in the last years.) Spending the next 6 months to a year trying to lower cholesterol levels by lifestyle interventions and reduce risk naturally is not playing with fire and risking your life, like some would have you believe. You’re talking about maybe dealing with a 0.5-2% increased absolute risk over the time while you’re trying to fix yourself. It’s a very reasonable, low time preference approach to your health. The alternative is taking a medication that directly impairs the most important cellular function necessary for life.
On this same note, strong recommendations for starting a statin are when that 10-year cardiovascular risk rate reaches 10%. For some people, 10% may be an acceptable risk level compared to starting a statin. 15% may be an acceptable risk level. Everyone will have a different personal preference and risk tolerance level. Guidelines are helpful, but not imperative to enforce on everyone. Most people are willing to start a medication based on guidelines without ever really knowing the basis for the guidelines because they’re never told. Most doctors don’t have a strong knowledge of the reasonings and especially statistical calculations behind recommendations. Pharmaceutical companies like it that way. In fact, pharmaceutical companies, along with other big industry players, provide significant funding for the various organizations making these recommendations. In 2020-2021 the American Heart Association received over $180 million in funding from pharmaceutical companies and other corporate entities5. This is in addition to the almost $357 million dollars spent by the pharma lobby in DC over the same period. Do you think these dollars are being spent to make sure Americans get the best information regarding their health? Keep in mind, Goldman Sachs (a large investment firm that holds significant influence over many of these companies) stated in their most recent industry report that curing disease is not a sustainable business model. Creating disease is very profitable, though. That’s the quiet part they don’t say out loud. Not to cast aspersions, but this may be why the AHA’s heart healthy check mark appears on some of the most sugar-filled and unhealthy cereal boxes and other foods in the grocery store.
Metformin
Metformin is a widely prescribed drug for the treatment of diabetes. It is the 8th most prescribed drug in America. It also directly acts on mitochondria, but this is part of its primary mechanism of action for its glucose lowering effects, rather than a side effect, as with statins.
Briefly, metformin disables the first step in the ETC, which significantly impairs energy production. Because the cells are then low on energy, they start to pull more sugar out of the blood stream in an attempt to generate more, and also start to use fat for energy production. This produces positive overall affects in people with chronically high blood sugar. Since the ETC is not properly functioning, metformin also results in less ROS in the cell, and less chance for damage to DNA or other organelles. Metformin may also increase mitochondrial biogenesis, increasing the density of mitochondria in certain tissues, which is generally beneficial.
While the goal of health, and essentially the definition of life, is to maintain self-regulated homeostasis, not all drugs are equally bad. The first step in treatment should always be via negativa, or removing the cause of harm, but if something must be added to restore equilibrium, it is essential to understand risks and benefits. It’s probably not surprising to find that metformin comes from the compound guanidine in the Galega officinalis plant, which has been used for centuries to treat symptoms now known to be associated with diabetes, like frequent urination. We also don’t completely understand the actual mechanism of action by which metformin works. This is an excellent encapsulation of the theory behind Medicine Across Space and Time. Empirical knowledge of the beneficial qualities of this drug have been known for centuries, rigorously tested through the gauntlet of time, and does so with an elegant complexity that evades our scientific investigations.
Metformin is far from perfect. Its active compound was discovered in a flower, isolated, synthesized, and now mass manufactured. Taking a tablet of metformin is far more potent than chewing on some goat’s rue (the common name for Galega officinalis), but metformin has several negative side effects as well, most commonly gastric discomfort and diarrhea, and the extremely rare but severe lactic acidosis. Again, treatment should be through removal of the cause, but when additive intervention is needed, it shouldn’t necessarily be done with the strongest medication, but with the one with the fewest negative side effects.
Compare metformin to statins, which were discovered in the 1970s in a lab in Japan. It was a systematic, top-down approach screening thousands of fungi that allowed Dr. Akira Endo to identify compactin, a compound that inhibits HMG-CoA reductase, an enzyme that is essential in the synthesis of cholesterol in the body. As discussed above, this also inhibits the production of CoQ-10 and has other deleterious effects on mitochondria. Based on this discovery, Merck & Co. soon identified a similar compound and proceeded to mass manufacture. While potent, it unquestionably does harm, and the high rate of reported statin side effects don’t even include all the second order effects associated with impairing the body’s fundamental energy production process. A top-down process will never properly account for unintended second order consequences in the way that a bottom-up process will.
NSAIDs and Others
Although many NSAIDs, such as Advil and Aleve, are available over the counter in the US, they are far from benign. NSAIDs are anti-inflammatory medications and primarily work by inhibiting cyclooxygenase enzymes and decreasing prostaglandin synthesis, but they also affect mitochondria. NSAIDs are a broad category of medications, so these effects are generalizations, but they can inhibit complexes in the ETC, increase ROS, and even directly damage mitochondrial DNA.
There are many other medications that affect mitochondria but are far less common. These medications include tetracycline antibiotics (doxycycline), anti-seizure medications (valproic acid), antipsychotics (haloperidol, olanzapine, clozapine, risperidone), anesthetics, and other.
Conclusion
Production of energy at a cellular level is essential to life, and mitochondria are central to this process. Working from first principles, in order to maintain health and vitality it is imperative to optimize mitochondrial function, and even more importantly, avoid impeding their functioning. For something so important to life, we spend very little time truly thinking about how substances we ingest affect them. Because mitochondria are so fundamental, the second-order effects of damage are widespread and underappreciated. Many of the effects of their malfunction are generalized, ambiguous and difficult to pin to an exact cause, i.e., “feeling tired”. You don’t need to understand in great detail how mitochondria work, but it you do need to understand what can be damaging to them, and in turn, your health.
Citations
1. Exercise and Mitochondrial Function: Importance and Inference- A Mini Review, by Vaishali et. al.
2. Exercise training increases mitochondrial biogenesis in the brain, Steiner, et. al.
3. Iron supplementation improves endurance after training in iron-depleted, nonanaemic women; Hinton, et. al.
4. Coenzyme Q10 and Its Impact on Exercise and Sport Performance in Humans: A Recovery or Performance-Enhancing Molecule?; Drobnic
5. AHA website https://www.heart.org//media/Files/Finance/21_22_Pharma_Funding_Disclosure_0323.pdf